The ‘Bill of Rights’ was developed at a workshop on 'The terminally ill patient and the helping person' in Lancing, Michigan by Dr Amelia Barbus1:
- I have the right to be treated as a living human being until I die;
- I have the right to maintain a sense of hopefulness, however its focus might change;
- I have the right to be cared for by those who can maintain a sense of hopefulness, however, this might change;
- I have the right to express my feelings and emotions about my approaching death in my own way;
- I have the right to participate in decisions concerning my care;
- I have the right to expect continuing medical and nursing attention even though ‘cure’ goals must be changed to ‘comfort’ goals;
- I have the right to not die alone;
- I have the right to be free from pain;
- I have the right to have my questions answered honestly;
- I have the right to not be deceived;
- I have the right to have help from and for my family in accepting my death;
- I have the right to die in peace and dignity;
- I have the right to discuss and enlarge my religious and/or spiritual experiences, whatever these may mean to others;
- I have the right to expect that the sanctity of the human body will be respected after death;
- I have the right to be cared for by caring, sensitive, knowledgeable people who will attempt to understand my needs and will be able to gain some satisfaction in helping me face my death.
Death is a process and not a single moment – a process which sometimes happens fast and other times more gradually. Quite often, radical changes in lifestyle must be made as there is movement from health to illness to dying.
This process is complex as it involves much more than just the physical experience of illness. It also includes emotional, social, spiritual, and cognitive experiences.
Culture and end-of-life within the context of psychosocial care
Each culture has its own dominant beliefs which influence the thinking and behaviour of the members of that culture. These beliefs also shape approaches to loss, illness, death and dying, choice of treatments, including the use of medications. In addition, each family/clan/group has its own practices.
Ethical principles have to be considered in the context of the traditions and belief-systems of the particular family seen by a psychosocial professional and as long as the patient is medically competent, to respect their wishes.
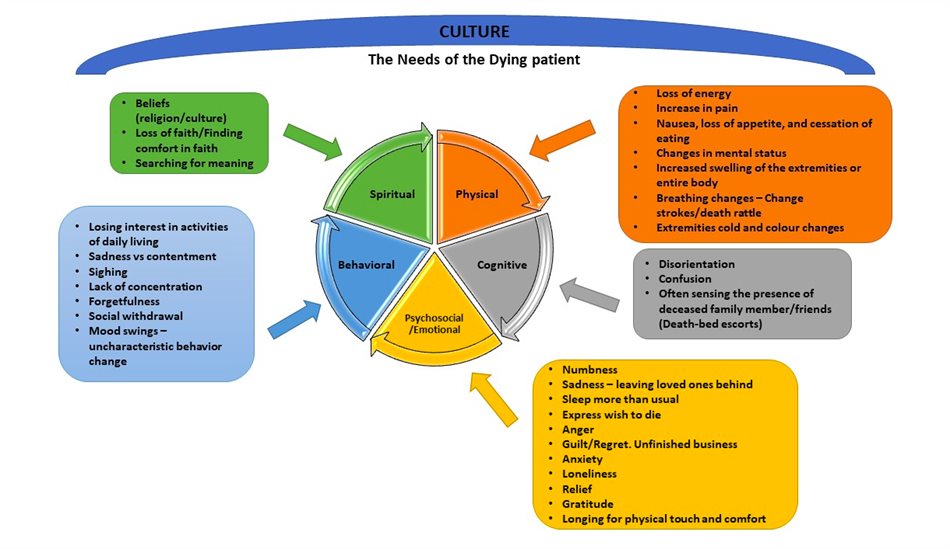
The patient’s personality, his/her strengths, and available resources also influence the patient’s needs. The visual below lists the needs of a dying patient. The umbrella ‘culture’ indicates how culture and belief systems will influence these needs, and each element will be impacted on by the social and cultural context of the patient.
Family structures and the right to know
Psychosocial services to the patient’s family play an important role that includes working with family members to validate and support the emotions experienced and link to community resources for additional psychosocial assistance if needed. These services may help prevent family breakdown or any long-term effects on the health and well-being of members of the family during the patient’s illness and into bereavement.
With permission from the patient, the psychosocial professional answers all the family’s questions honestly and explains what is happening through the progression of the patient’s illness. When there is a large family, it is necessary to find out if all members are to be informed or only certain members. The psychosocial professional encourages communication between patient and family and by way of supporting the dying patient’s Bill of Rights, will also encourage them to respect the patient’s wishes regarding choices of treatment and care.
Personal ethics and values and the professional
Self-reflection and self-awareness for psychosocial professionals in palliative care is critical to avoid any unintended self-values being projected onto a patient. Ethical principles, medical best practice, legislation and the ‘Dying person’s Bill of Rights’ guide the practice of all professionals working in palliative care as well as decision-making regarding treatment and care. Ethical practice is integral to the care and support provided by the psychosocial practitioner, both professionally and personally. It has to be within who they are and their way of being with patients and families.
If you have missed the last two articles in this series of three, follow these links:
This series contains information from the Hospice Palliative Care Association (HPCA) Psychosocial Palliative Care Course manual. Online courses take place regularly, with the next courses planned for 24 July and 11 September 2023. For more details, visit: https://bit.ly/3nSpN1X.
1Barbus, 1975